
inside MSF treatment centers during the Ebola outbreak in DRC
Weeks after Ebola resurfaced in the Democratic Republic of Congo and Uganda, Médecins Sans Frontières (MSF) has ramped up efforts to curb the spread. Our teams invite you into their treatment centers in Goma and Bunia, Ituri province—the outbreak’s epicenter—where they are battling the country’s seventeenth epidemic.
Epidemiological toll continues to rise
With expanded testing in late May, the DRC Ministry of Health updated its figures. As of June 4, 2026, the National Institute for Biomedical Research (INRB) reported:
- 381 confirmed cases;
- 64 confirmed deaths;
- 233 suspected cases currently isolated.
In Uganda, authorities are monitoring 19 reported cases and one death as of June 5.
MSF expands and reopens Ebola treatment centers
To halt the spread of Bundibugyo virus and break transmission chains, MSF is adapting its response in the hardest-hit areas.
In Bunia: a center stretched to the limit
Bunia’s treatment center is overwhelmed. By June 5, it housed 37 suspected and 7 confirmed patients. To reduce risks, expansion is underway. “We’re clearing a new plot and will double capacity to 70 beds within days,” says Anthony Kergosien, MSF Emergency Coordinator in Bunia. If needed, the center can scale up to 100 beds.
View this post on Instagram
Goma: reopening a historic center
In Goma, MSF has reopened a dedicated treatment center to isolate suspected cases and care for confirmed patients. The first admissions began on May 28.
“This center was used during previous outbreaks. Teams start by talking to patients, reassuring them about the process, explaining care protocols, average stay duration, and sample collection,” explains Tathy Modjaka Nzoko, MSF Medical Activity Manager in Goma.
View this post on Instagram
Protecting healthcare workers and earning community trust
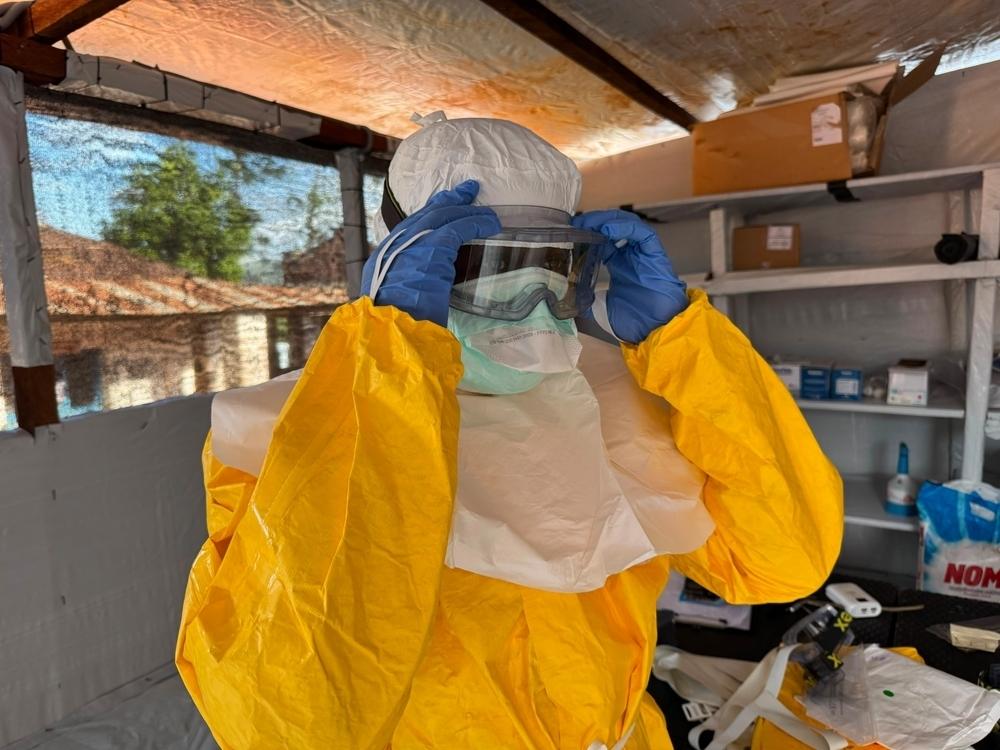
Safeguarding frontline staff
Medical teams wear full personal protective equipment (PPE) to shield themselves from Bundibugyo virus. The virus’s low infectious dose makes protection critical. “A few viral particles in the eyes or mouth can spark infection,” warns Armand Sprecher, MSF Emergency Physician and Epidemiologist.
PPE must be fluid-resistant since the virus spreads via bodily fluids. “Unlike previous outbreaks, we lack approved vaccines and treatments, making PPE our first line of defense,” he adds.
Winning community confidence
Encouraging patients to seek care immediately hinges on trust. “Local trust in MSF is vital. Families traditionally care for sick relatives at home, but we need them to come to treatment centers right away. The PPE can look alien, making some hesitant. We explain that many responders wearing this gear are people they know,” Sprecher notes.
View this post on Instagram
Training local teams and sharing expertise
Scaling up the response relies on knowledge transfer. Before deployment, teams undergo specialized training at a center in Belgium. “Every Ebola outbreak underscores the value of knowledge sharing. MSF relies on experts with firsthand epidemic experience, who train others or guide field teams,” Sprecher explains.
Understanding Bundibugyo virus: key facts about this outbreak
Unlike prior waves in DRC, this outbreak stems from the Bundibugyo Ebola virus (part of the orthoebolavirus family, which includes Zaire and Sudan strains).
While the fatality rate for Bundibugyo (25–40%) is lower than classic Ebola, the response faces a major hurdle: no approved vaccines or treatments exist for this strain.
MSF’s ongoing humanitarian mission
Hundreds of MSF staff remain active in Ituri and North Kivu, with new isolation capacities being set up in South Kivu. Weekly, several tons of medical and logistical supplies arrive from international hubs to support the intervention.


